Guide helps parents recognize teen stress signs, triggers, and impacts. It highlights benefits of counselling, professional support by Melbourne psychologists, and services by Your Mind Matters, including telehealth.
This guide clarifies differences between ADHD and anxiety in children, highlighting symptoms, impacts, and the importance of early professional assessment for accurate diagnosis and effective support.
We have all had moments where we have felt overwhelmed and dysregulated. Swamped by big feelings and emotions, it can feel like they have control of our body, rather than the other way round. For children, this can be a particularly scary experience, and they can struggle to calm down. Teaching children about how their brains work is an important step in gaining mastery over our emotions. Knowledge is power!!
It can be helpful to think of your brain as like a house. There’s an “Upstairs” and “Downstairs” part.
The Downstairs part (Brainstem and Amygdala) looks after our basic survival functions. The Downstairs part is intact at birth. It is responsible for:
Regulating breathing and heart rate
Sensory processing
Sensing threat
The Upstairs Part (Prefrontal Cortex) is our “thinking brain”. Fun fact parents – it’s not fully developed until you’re about 25, so it’s under construction for most of childhood and adolescence and is shaped by experience. It’s responsible for:
Logic and reason
Problem solving
Making decisions and managing emotions
When we are calm, ready to learn, play and socialise with others, our Upstairs and Downstairs brains are communicating well. The Upstairs brain is in charge, and it can THINK before it ACTS.
But when we feel stressed, angry, or upset, our Upstairs and Downstairs brains stop communicating well. The Downstairs Brain REACTS before we THINK. When the Amygdala perceives threat, it activates a fight/flight/freeze response in the body (depending on the environment we are in and our temperament). Recent research suggests that we may utilise a fawn response as well (people pleasing). The Downstairs brain channels adrenaline, and makes us super strong, super fast and REACTIVE. This often leads children to meltdown or to become dysregulated, as they are overwhelmed by stress. In this state, it is very hard to think clearly, and it becomes the role of parents and teachers to help the child to regulate.
So, what can we do?
Recognising signs of stress early allows us to manage our feelings, utilise strategies and regulate our emotions. In therapy, children learn to identify their emotions and associated body symptoms and develop strategies to manage stress and anxiety. Having movement breaks or moments to recharge throughout the day, and utilising strategies, can help us with managing the build-up of stress in the body and increase our coping capacity for when we do have big feelings and emotions.
Sometimes, especially for younger children, it’s overwhelming when big feelings and emotions are triggered. If a child is dysregulated and highly stressed, the first goal is to regulate (calm heart rate and breathing, help the child to access the Upstairs Brain).
Parents and teachers can help by:
Keeping calm and connect! Make eye contact, move down to their level, and use a soothing tone and body language to communicate empathy. Empathic statements that reflect how a child is feeling, and NAMING the emotions/feelings they are experiencing, can help to regulate the brain and move it from a REACTIVE to a REFLECTIVE state.
“I can see you’re feeling angry, it didn’t go the way you expected.”
“You’re really upset that your friends hurt your feelings.”
“You’re feeling scared at trying something new.”
Redirecting to a calm space or activity to help soothe. A calm space such as a child’s bedroom or the trampoline can offer a space for the child to soothe and reduce sensory overwhelm. You can stay nearby and offer the child a chance to reconnect when they’re ready and feeling calmer.
Setting safe limits to ensure everyone’s safety. Naming the feeling and setting limits on unsafe behaviour – offer viable alternatives to allow the child to express the emotion/feeling they are experiencing in a safe manner.
“I can see you’re mad, I won’t let you hit me. You can hit the beanbag, or the cushion.”
Remember: You can’t pour from an empty cup!
If you are feeling stressed or dysregulated yourself, it’s okay to take a moment to step away and allow yourself space to calm down. We cannot co-regulate a child if we don’t feel calm and regulated ourselves. We want to RESPOND calmly, rather than REACT. Parenting is hard work, and it’s important to be self-compassionate.
The Power of Repair:
And once a child is calm, there’s the opportunity for REPAIR and learning. We all make mistakes and have reactive moments, even as adults. Offering your child a chance to repair the relationship, strengthens your connection and helps model healthy communication. It also helps build self-esteem and reduce the shameful feelings associated when we feel we have “messed up”.
“Hey I was wondering about how you were upset yesterday. I wonder if you were feeling this way because…….. Sometimes I feel that way too. I wonder what we could do differently next time? I love you and we can work through this together.”
Further Resources:
Dan Siegel and Tina Payne Bryson – The Whole Brain Child
‘If you would like to learn more about developing emotional regulation for children, or upskill as a parent in coregulation skills, our team are here to help! Call us now and take that first step towards a calmer family life.
This blog was written by Shivonne Cammell – Senior Accredited Mental Health Social Worker at YMM.
Shivonne completed her undergraduate degree in psychology and neuroscience at Monash University, followed by a Master of Social Work at University of Melbourne.
Shivonne specialises in utilising play therapy to help children recover from trauma and grief, develop resilience, enhance family relationships, and adjust to new social circumstances in positive ways. She also has experience working with adolescents and adults to address issues including anxiety, low mood and depression, low self esteem and interpersonal difficulties.
Shivonne is a warm and approachable clinician, who works from a strength-based approach incorporating methodologies including cognitive behavioural therapy, acceptance and commitment therapy, interpersonal therapy, and relaxation and mindfulness strategies.
Pathological demand avoidance, or Pervasive Drive for Autonomy (PDA)*, is an anxiety-driven need for control and resistance to demands/expectations that threaten a sense of autonomy. Whilst everyone experiences demand avoidance at times (e.g., refusing to complete homework or household chores), for individuals with PDA, everyday demands such as “put on your shoes” or “take a shower” can cause significant anxiety and evoke extreme emotional reactions (panic attacks or meltdowns). In fact, individuals with PDA may resist demands even if it’s something that they enjoy or want to do. It is the expectation, rather than the nature of demands, that leads to a perceived lack of control. Thus, demands that may trigger PDA include:
Direct Demands: Instructions e.g., Brush your teeth, put your shoes on, do your homework, corrections, or discipline.
Indirect Demands: Praise, discussions/comments about the future, transitions, social expectations.
Internal Demands: Hunger, thirst or needing to use the bathroom.
Wants/desires: Hobbies/interests, special occasions.
*Pervasive drive for autonomy is the preferred name for many within the autistic community.
So, how do we identify individuals with a PDA profile?
Core Features of a PDA Profile
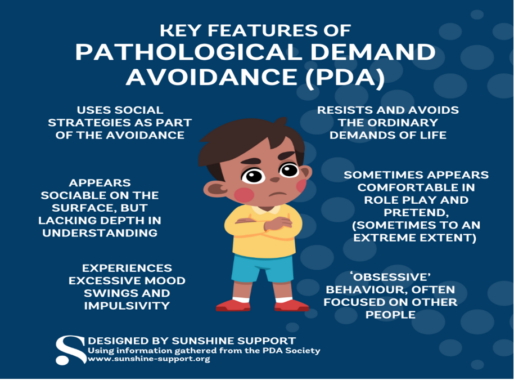
At present, PDA is not included in the International Classification of Diseases (ICD-11) or the Diagnostic Statistical Manual (DSM-5-TR) as a formal diagnosis. Rather, PDA is currently considered a profile of autism characterised by:
Resistance/avoidance to ordinary demands of life and use of “social strategies” to regain autonomy:
PDAers may employ various social techniques as a means of avoiding demands, including:
Distraction: Giving compliments, changing the subject, feigning injury, mimicking.
Controlling the actions of others around them: “You do it”, suggesting alternatives.
These behaviours can often be misinterpreted by others as manipulative. When distraction, control and avoidance strategies fail, anxiety levels are heightened, and distress escalates, which can lead to aggression (hitting, kicking, biting), elopement, or self-harm. It is important to note that these behaviours are not deliberate; rather,PDAers experience panic and a fight/flight/freeze/fawn response.
PDAers may present with less obvious differences in social communication and understanding than other autistic children. They may have strong verbal fluency and exhibit more eye contact. However, they may also struggle with understanding social hierarchy, e.g., wanting to be co-teachers or co-parents, and have a preference for being in control during play.
Other key characteristics include:
Intense emotions or mood swings
Comfort in role-playing and storytelling
Intense focus on interests, often directed at other people
Pathological demand avoidance can present differently depending on the setting and an individual’s capacity for demands at any one time. In school, a PDA child may refuse to start tasks or engage in distracting behaviours to avoid work. At home, they may have frequent meltdowns about routine tasks such as taking a shower or getting dressed.
So, how can we support individuals with PDA?
Strategies to Support PDA Children
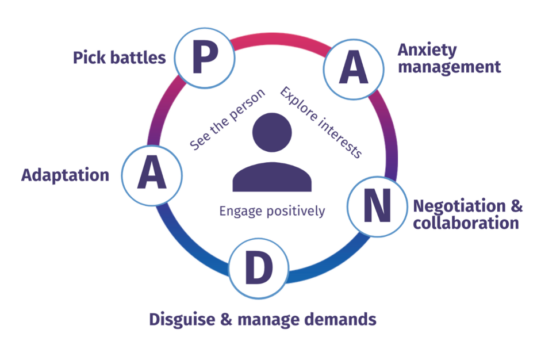
It is important to understand that PDA behaviour is driven by anxiety and that PDAers respond to demands as if they are a direct threat to their safety or well-being. Thus, low arousal approaches that reduce anxiety and provide a sense of control are essential for supporting PDAers. The Pathological Demand Avoidance Society recommends an approach that is flexible, based on trust, and collaborative. This is called the PANDA approach, as outlined below.
Image by PDA Society UK
Pick Your Battles:
Minimise non-essential rules and agree on non-negotiable boundaries – Ask yourself what rules are important for the child, family or class. Prioritise rules as high, medium or low priority.
Allow for some choice/control by providing two options or allowing “no” as a response.
Provide explanations.
Manage Anxiety:
Recognise and respond to the child’s cues that they are becoming overwhelmed or stressed.
Reduce uncertainty.
Treat distressed behaviours as panic attacks and support throughout
Recognise that when in a heightened state, a child is not fully in control of his or her behaviour, as the emotion centre of their brain takes over.
Negotiate/Collaborate:
Keep calm
Proactively negotiate
Disguise Demands:
Reframe requests – Instead of using words such as “need”, “must” “wont” “can’t” or “it’s time to” try using phrases such as “is it okay with you” “how do you feel about”, “I wonder.”
Use declarative language, e.g., “The clothes are on the bed.”
Disguise demands as challenges – “I bet I can get my coat on first”.
De-personalise the request, e.g., “it’s the school rules.”
Adapt:
Use humour, novelty, distraction, and roleplay.
Be flexible and have a plan B.
Be cautious with rewards or praise:
Rewards charts can create additional demands if the original demands are not achieved. Instead, try providing spontaneous rewards.
Praise or encouragement can be perceived as a demand; instead, try providing praise indirectly or focusing on the process. When offering encouragement, provide choices or exit strategies.
Resources
If you’d like to learn more about PDA and how it presents, please see the following:
Understanding Pathological Demand Avoidance Syndrome in Children: A Guide for Parents, Teachers, and Other Professionals by Phil Christy, Margaret Duncan, Ruth Fiddler, and Zara Healy.
Me and My PDA: A Guide to Pathological Demand Avoidance for Young People by Gloria Dura-Vila and Tamar Levi.
The Educator’s Experience of Pathological Demand Avoidance by Laura Kerbey
If you’re noticing patterns of demand avoidance in your child or would like some help supporting individuals with a PDA profile, please feel free to contact our admin team on 9802 4654.
This blog was written by Michaela Hughes – Psychologist at YMM.
Michaela has a special interest in working with children and young people with a range of neurodevelopmental disorders including Autism Spectrum Disorders (ASD), ADHD, Intellectual Disability and Language Impairment.
Michaela believes in a warm, empathetic, and collaborative approach to the therapeutic process and that treatment should be tailored to the client’s individual needs. She strives to adopt a client-centred approach, drawing on a range of evidence-based treatments including cognitive behavioural therapy, play-therapy and mindfulness-based therapy.
Have you ever experienced the challenge of navigating a teenager’s sudden outbursts or trying to calm a younger child’s meltdown in a crowded store? It’s a common scenario for many parents.
Understanding why the challenging behaviour occurs
Psychologist Ross Greene’s Collaborative & Proactive Solutions (CPS) approach emphasises that if they could do well, they would do well.
Understanding why children exhibit challenging behaviours is the first step toward effectively managing such behaviours. No child wakes up and decides that they want to do ‘bad’ things or have a meltdown in front of all of their friends! Fundamentally, all children want to do well, and it is up to parents and caregivers to try to understand why they are engaging in behaviour that interferes with their ability to meet expectations at home, school or in the community.
Often, children with behavioural challenges are labelled negatively. Let’s have a look at some of these all-too-common terms…
‘They’re attention seeking!’.
This label identifies an unmet need in the child’s life but offers limited solutions. It implies that the child is acting with intention.
‘They’re manipulative!’
Children engaging in challenging behaviours do so impulsively, emotionally and without much forethought. Competent manipulators possess many skills, such as planning, impulse control, and organisation.
‘They’re unmotivated!’
This label doesn’t capture what is going on with a child and may create low self-worth, leading to further challenges in the future.
‘They’re testing the limits!’
This often leads parents to prioritise compliance over understanding and addressing factors contributing to behaviours.
Children may lack the skills to behave appropriately. They may have unsolved problems or even unmet needs contributing to their behaviour. Adults can help by collaboratively finding the cause of their child’s challenging behaviours and helping them implement strategies.
Image by Nichole Schlechter on https://nicoleschlechter.com
Managing challenging emotions and behaviour
When a child is struggling to regulate their emotions, their ability to engage in problem-solving and collaboration is compromised.
The Zones of Regulation framework provides a systematic approach to help children understand and manage their emotions and behaviours. By categorising emotions and states of alertness into four colour-coded zones – Green, Blue, Yellow, and Red – children learn to recognise and label their feelings, gaining awareness of their current emotional state.
Techniques such as deep breathing or taking a break may help young people calm down in the Red Zone, while activities like visualisation or positive self-talk can help them shift back to the Green Zone.
It is essential for parents to remember that when a child is engaging in unsafe, challenging behaviours, the critical goal is always de-escalation. No learning occurs when a person is dysregulated. The team of child clinicians at Your Mind Matters can support children and their parents in learning to use de-escalation strategies to calm their bodies and minds.
This poster was put together by Elina from Your Mind Matters but is based on information from https://zonesofregulation.com/. Have you seen the movie Inside Out (PG ages 6+) to recognise these characters?
Teaching adaptive behaviour and skills
In addition to emotion regulation, it’s essential to teach children adaptive behaviours and skills that will help prevent future challenges, according to Ross Greene’s Collaborative & Proactive Solutions (CPS). Children who demonstrate challenging behaviours already receive negative natural consequences for their behaviours. Giving them more consequences and punishing them (e.g. detentions, removing favourite toys, yelling) does not give them the skills to succeed and instead may just further harm their self-esteem.
What interventions DO solve problems and teach skills?
Identifying situations where the child’s skills are consistently lacking:
E.g. Your child yells and cries when they lose
Implement a cool-down routine.
E.g. A go-to activity to regulate emotions when upset.
Teaching the child practical ways to improve their skills:
E.g. Teach the child how to recognise physical signs of anger and disappointment.
E.g. Teach coping strategies like self-talk
Remove barriers that impact the child’s success:
E.g. Modify the game to reduce the emphasis on winning/losing.
Practise, practise, practise!
E.g. Role playing different reactions to losing a game.
Provide accommodations:
E.g. Allow for mistakes and setbacks and be flexible in your approach as the child learns the new skill.
Managing challenging behaviours in children and teens can be a daunting task, but parents and caregivers do not have to navigate it alone. Every child is unique, and finding the right strategies may take time and patience. If you would like support in parenting a child with challenging behaviour, our team of clinicians can help.
Additionally, if you are interested in learning more about Ross Greene’s CPS model to working collaboratively with children and teens, you may enjoy his lecture below:
This blog was written by Elina Makela – Psychologist (Educational and Developmental Psychology Registrar) at YMM.
Elina is passionate about helping young people presenting with behavioural and emotional difficulties. Elina works collaboratively with families to support young people with developmental difficulties related to Autism Spectrum Disorder (ASD) and Attention Deficit Hyperactivity Disorder (ADHD). She also has a strong interest in working with young people who experience eating difficulties, poor body image, sleep issues, and anxiety. Through warmth, compassion and play, Elina creates rapport with her younger and adolescent clients.
“Enter into children’s play and you will find the place where their minds, hearts, and souls meet.” -Virginia Axline
What is Play Therapy?
Play Therapy is an effective and appropriate way to help children aged 2-12 years work through emotional, psychosocial and behavioural difficulties. It can help address issues faced in the family, school, or interpersonal relationships. This technique works for children like counselling or psychotherapy does for adults.
Play Therapy is based upon the fact that play is the child’s natural medium of self-expression. In Play Therapy a child is given the opportunity to ‘play out’ feelings and problems just as an individual in adult therapy may ‘talk out’ their difficulties.
In Play Therapy, a relationship develops between the child and the therapist, where the therapist enters the child’s world, following the child’s lead, to develop a safe place and a relationship of trust, empathy and acceptance. Within this context, children are then free to express feelings, thoughts, experiences, and behaviours through play. Toys are used like words and become the child’s natural language. Children are encouraged to make choices, to explore possibilities and to develop resilience and self-actualisation, with a skillful therapist trained to respond therapeutically.
Who is Play Therapy for?
Play Therapy can assist children aged 2-12 years experiencing difficulties such as:
Child abuse and neglect
Developmental trauma
Grief and loss
Relationship and social issues
Adjusting to family changes such as separation and divorce
Social issues – difficulties with friendships, social skills
Emotional regulation issues
Anxiety
Selective mutism
Chronic illness or medical trauma
Benefits of Play Therapy:
Play Therapy provides a safe and therapeutic environment for children to explore and learn about themselves and their world, to build confidence and self-esteem, whilst working through the issues that may have hindered their development so far.
Play Therapy helps children to find healthier ways of communicating and to develop a greater sense of identity and self-esteem, while increasing their emotional intelligence and resilience.
Evidence based literature supports the effectiveness of play therapy, with research replicated with different cultural groups and demographics.
History and Adaptations of Play Therapy:
Virginia Axline originally developed Child-Centered Play Therapy as a methodology based on key principles of the person-centred approach, with primary focus on the relationship between child and therapist being based on genuineness, acceptance and trust. This created a safe and trusting environment for children to explore and examine all emotions and experiences at their own pace, and to integrate them. The therapist works with the child to provide empathy and unconditional acceptance, to help the child to feel understood, so they in turn can gain a sense of mastery and understanding of their own experiences.
In the 1960s, Bernard and Louise Guerney developed Filial Therapy, an adaptation of Play Therapy where parents were taught Child-Centered Play Therapy skills so that they could facilitate therapy sessions with their children. This model recognised the influential impact of parents in assisting their children’s healing and growth. Landreth refined this model into a 10-session structured program known as Child-Parent Relationship Therapy, an evidence-based model focused on strengthening the parent–child relationship and helping parents to better understand and respond to their children’s social, emotional, and behavioural needs.
Modern day Play Therapy incorporates many different methodologies adapted to the child’s age and stage of development, presenting issues, and stage of therapy. These can often incorporate structured or unstructured play, storytelling, art techniques, games and sand tray. The goal is still to provide an accepting and open environment for a child to feel safe to express their feelings, but techniques may utilise directive strategies as well.
If you would like to learn more about play therapy and how your child can benefit from this counselling approach, our team of clinicians can help.
References:
Axline, V. (1967; republished 1989). Play therapy: The inner dynamics of childhood. New York: Ballantine Books.
Bratton, S. C., Landreth, G. L., Kellam, T., & Blackard, S. R. (2006). Child parent relationship therapy (CPRT) treatment manual: A 10-session filial therapy model for training parents. Routledge/Taylor & Francis Group.
Cochran, N. H., Nordling, W. J. & Cochran, J. L. (2010). Child-centered play therapy: A practical guide to developing therapeutic relationships with children. New Jersey: John Wiley & Sons.
Landreth, G. L. (2012). Play therapy: The art of the relationship. New York: Routledge.
This blog was written by Shivonne Cammell – Senior Accredited Mental Health Social Worker at YMM.
Shivonne completed her undergraduate degree in psychology and neuroscience at Monash University, followed by a Master of Social Work at University of Melbourne.
Shivonne specialises in utilising play therapy to help children recover from trauma and grief, develop resilience, enhance family relationships, and adjust to new social circumstances in positive ways. She also has experience working with adolescents and adults to address issues including anxiety, low mood and depression, low self esteem and interpersonal difficulties.
Shivonne is a warm and approachable clinician, who works from a strength-based approach incorporating methodologies including cognitive behavioural therapy, acceptance and commitment therapy, interpersonal therapy, and relaxation and mindfulness strategies.
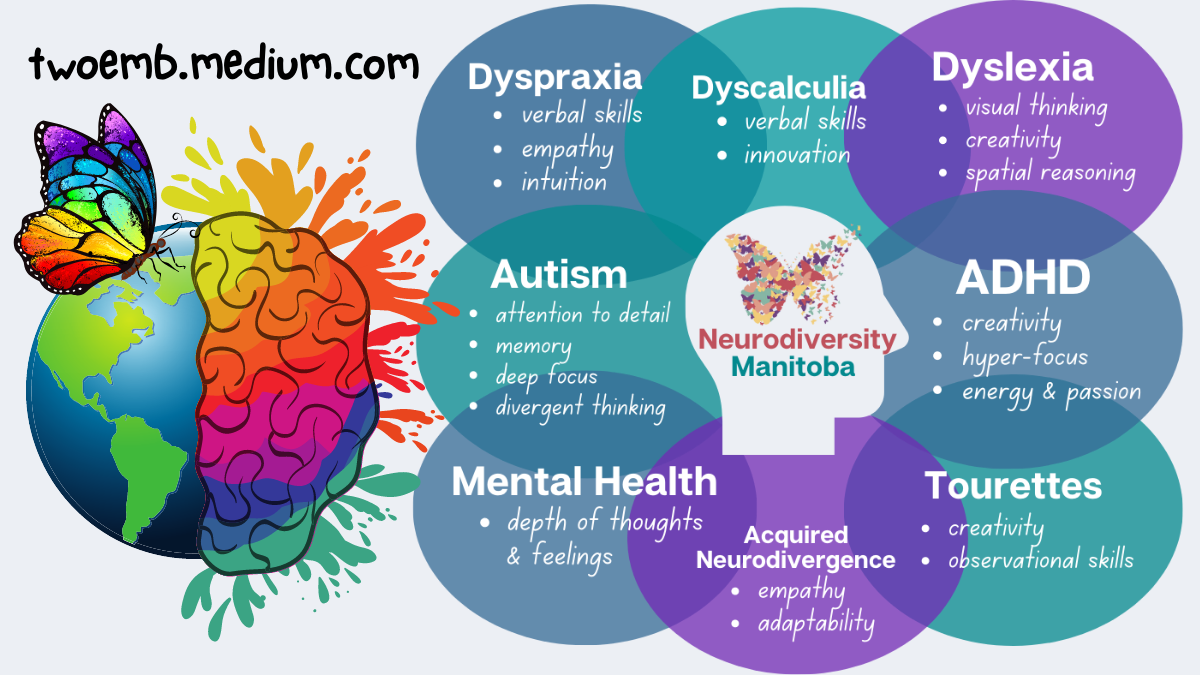
In recent years, the neurodiversity movement has become increasingly prominent. Coined in the 1990s by Australian sociologist Judy Singer, the concept of neurodiversity acknowledges and embraces neurological differences i.e., variations in the way in which individuals interpret, process, and learn information. Neurodiversity can be broken down into two subgroups of individuals: those who are neurotypical and those who are neurodivergent.
Neurotypical describes individuals who think and process information in ways “typical” for their culture.
Neurodivergent refers to individuals whose brain functioning differs from what is considered “typical.” This encompasses people with a range of conditions including:
So, what does it mean to be neurodiversity affirming?
A Neurodiversity Affirming Approach
In contrast to a deficits-based approach which focuses on “fixing” the impairments associated with neurodevelopmental conditions, a neurodiversity-affirming approach acknowledges that all neurotypes have unique strengths, interests, and support needs. Moreover, this approach highlights the role of the environment and societal barriers in further exacerbating challenges faced by neurodivergent individuals.
Traditional therapeutic approaches to working with neurodivergent individuals have focused on encouraging individuals to mask neurodivergent traits such as reducing stimming behaviours or forcing eye contact and mimicking neurotypical styles of communication. However, emerging evidence suggests that these practices can lead to shame, anxiety, depression, and reduced self-worth (Sedgewick et al., 2021). Rather than perpetuating the idea that neurodivergent individuals need to mask certain characteristics, neurodiversity-affirming practice seeks to understand and inform individuals about differences and provide adaptations and supports that affirm neurodivergent identities. Subsequently, this can lead to self-advocacy regarding accommodations within the classroom or workplace and help cultivate a sense of self-esteem.
So, what does this look like in therapeutic practice?
Neurodiversity-Affirming Therapy
The goal of neuro-affirming therapy is to embrace the uniqueness and strengths of neurodivergent children and provide them and their families with the skills, tools, and strategies to allow for improved participation within the home, school, and play environments. This may involve:
Seeking to understand the needs of neurodivergent children from their perspective and adapting the environment to meet these needs.
Understanding and respecting neurodivergent communication styles.
Understanding and accommodating individual sensory needs.
Encouraging neurodivergent rather than neurotypical listening skills.
Assisting in developing self-advocacy and problem-solving skills.
Teaching children to better understand the emotions, behaviours, and communication of other people around them, so they can better choose how they want to respond.
Validating children’s feelings, helping them recognize their triggers, and assisting in identifying calming strategies.
Recognizing the need for processing time and safe spaces.
Encouraging safe self-regulation skills, including stimming.
Adopting neurodiversity affirming language
Neurodiversity affirming therapy does not involve:
Promoting masking, loss of autonomy, or loss of personal agency.
Eliminating stimming behaviours.
Developing goals that seek to “cure” neurodivergent behaviours.
Neurodiversity Affirming Resources
If you’d like to learn more about neurodiversity or the neurodiversity-affirming approach, please see the following:
If you’re interested in seeking out neurodiversity-affirming support for yourself or your child or you’d like to know more information, please feel free to contact our admin team on 9802 4654.
References
Sedgewick, F., Hull, L., & Ellis, H. (2021). Autism and masking: How and why people do it, and the impact it can have. Jessica Kingsley Publishers.
This blog was written by Michaela Hughes – Psychologist at YMM.
Michaela completed her Masters of Educational and Developmental Psychology at Monash University, and her Honours at the University of Melbourne.
Michaela has a special interest in working with children and young people with a range of neurodevelopmental disorders including Autism Spectrum Disorders (ASD), ADHD, Intellectual Disability and Language Impairment.
Michaela believes in a warm, empathetic, and collaborative approach to the therapeutic process and that treatment should be tailored to the client’s individual needs. She strives to adopt a client-centred approach, drawing on a range of evidence-based treatments including cognitive behavioural therapy, play-therapy and mindfulness-based therapy.
Parenthood tends to be talked about in glowingly positive terms. It is described as a beautiful, natural part of life that is all sweetness and light. In this glowing description of parenthood, it is important to remember that having a baby is a big change in life and adapting to this change can be difficult. Having sad or difficult emotions during adapting to a new life does not make you a bad parent! You are not alone. Having a baby is a profoundly powerful experience, and intense experiences tend to create big emotional responses.
How are baby blues different to postpartum depression?
Postpartum Depression is not the same as the typical ‘baby blues’ that occur around day 4 post birth. Generally, the baby blues are due to the hormonal changes going on in your body after giving birth, but it does not tend to last more than a few days.
“Baby blues” may make you feel irritable, moody, weepy, restless, or unable to sleep – or all of the above. These feelings often tend to pass as you gain confidence and get into some routines. In postnatal depression, symptoms last longer than 2 weeks, may be more severe and often interfere with your ability to function normally. Unlike ‘baby blues’, postnatal depression doesn’t usually go away on its own. This can be especially tough to cope with when you are recovering from birth and have a new baby to look after.
Signs of postnatal depression
Postnatal depression, also known as postpartum depression, is a type of mood disorder associated with childbirth. There is no single cause of postnatal depression, but physical and emotional issues may play a role. Physical issues include hormonal changes after childbirth and sleep deprivation; while emotional issues include feeling overwhelmed/anxious and having money, work or relationship problems.
Some common symptoms of postnatal depression include:
Losing interest or lack of interest in your baby
Fatigue (a feeling of heaviness)
Hopelessness and sadness
Feeling overwhelmed
Sometimes extreme thoughts such as that of suicide or self-harm or harming your baby (if you are experiencing any of these symptoms or know of someone that might be, please seek help from a medical professional ASAP)
Who can I talk to for advice and support?
Talk to your partner, or someone else you trust.
Ask your GP, midwife or child healthcare nurse for advice.
Call one of these support services:
PANDA (Perinatal Anxiety & Depression Australia) — 1300 726 306
ForWhen — 1300 24 23 22 (Monday to Friday, 9.00am to 4.30pm)
If you are going through difficulties and need to find your inner strength, why not give us a call today? Our team of highly skilled and well-experienced Psychologists are here to help.
This blog was written by Aanchal Sood – Psychologist at YMM.
Aanchal completed studies in psychopharmacology and psychology in England, and is fluent in both Hindi and Punjabi.
Aanchal has experience assisting adolescents, adults and couples to address a variety of difficulties including anxiety and mood disorders, grief and loss, trauma and stress related disorders, adjustment issues (e.g. cultural adjustment), sleep difficulties, relationship difficulties, schizophrenia spectrum and other psychotic disorders, obsessive compulsive and related disorders.
Feel overly responsible for the emotional needs of others
Insecure about depending on others
Guilty in the face of attempting to prioritise your own needs
Struggle with drawing boundaries
Often feel like you are not doing enough for others
If you endorsed any of the above, could you have been a parentified child?
“Parentification” is the outcome of a role reversal, wherein a child finds themselves obliged to act as a parent to their own parent or siblings. Rather than the parent responding to the child’s emotional needs, the child feels compelled to take on the role of meeting the parent’s emotional needs. Consequently, the child becomes highly attuned to any changes in the parent’s mood. This can occur due to a variety of different situations, for example, in the face of divorce, where a parent turns to the child for ‘emotional unloading’, the child quickly becomes an ear for the parent’s distress, perhaps acting as an advisor or mediator. Basically, the parent inappropriately turns to their child to meet his or her own needs for affection, approval, reassurance, stability or control….
What a hefty burden for a child to bear, at any age! Often this results in the child maturing quickly and taking on the role of an adult way too early! Most of the time, in parentification there is no malicious intent, the parents love their child but with limited capacity and are driven by personal vulnerabilities.
As adults, these children would likely endorse the above questions. Whether aware of this process or not, they may refer to their parent as their “best friend”, “lifeline”, or “confidant”, however, often report feeling empty, smothered, and struggle with their sense of self-identity. While the personal impacts of parentification can be distressing, the role of caretaker can also provide a sense of control, certainty, and safety. It is often not until these adults reach a point of utter burn-out that the impacts of this role are considered.
So perhaps you have identified some of these themes in yourself and your relationship with a parent. If you have, a sense of anger and loss is completely understandable. If you are interested in starting your journey toward healing from parentification the below tips may be a good starting point:
Own/tell your story: As part of reclaiming elements of your lost childhood, that inner child needs to tell their story. Acknowledging your truth is the first step that will likely allow room for justified feelings of grief and anger. Therapy provides a non-judgemental safe space for your truth to be heard.
Prioritise your own needs: Often a deprivation of joy and play can accompany a parentified history. The good news is that you can become your own parent to your inner child and allow them to play, make a mess, and soak up the things that make their heart glad. It may take some time for you to connect with your needs so take it slow, it might be that you start off with prioritising some time for a hobby or activity that you don’t often get around to.
Self-compassion: Guilt is an emotion that is frequently felt by the parentified child and often this guilt does not fit the facts. Typically, the automatic default is to assume that things are their fault with the inner critic pushing them to do more for others. It’s time to extend yourself a kind hand and cultivate self-compassion.
Thank the inner critic: The inner critic that berates you with the “do more” and the “fix it” story formed as a coping mechanism in times of distress. Instead of leaning into the critic with contempt, it may be helpful to recognise the critic for their help but remind them that you have got it from here!
As with healing from any form of trauma, this will take time. Tread softly with yourself, nurture your needs, you deserve to! Psychotherapy can also provide a space for you to practice these skills and help you process your feelings along the way. Our team of psychologists are here to help.
References:
Interpersonal Process in Therapy: An Integrative Model- Book by Edward Teyber
This blog was written by Blair Raatjes, Psychologist at Your Mind Matters Psychology Services. She works with us 2 days per week.
Blair understands that seeking psychological help for the first time can be a nerve wracking experience for clients, therefore, she is committed to providing a warm, accepting and compassionate environment. She believes that collaboration, empathetic understanding, and respect are essential components to therapy and is interested in evidence-based approaches that emphasise the importance of catering to each client’s needs and strengths. Blair has experience using key therapeutic techniques, including Cognitive Behaviour Therapy and Motivational Interviewing and has a keen interest in Mindfulness based techniques such as Acceptance and Commitment Therapy.
As parents, it’s our desire to want to give our kids the best. We expect a lot from ourselves to be the best parent for them and hope that we are able to raise them healthy and well.
The way we parent our children is very much affected by how we were raised as a child. If we were ‘punished’ for experiencing and showing strong and intense emotions such as anger and frustration, we are more likely to react in the same way when our children express these emotions.However, that does not mean we can’t change or do things differently.
It is my opinion that there is no ‘one size fits’ all parenting style that will suit and work for every family. Nonetheless, there are some general rules of thumb that we can keep in mind to help us navigate our way through this journey called parenting.
1) Address the emotion first
Have you ever experienced being ‘lectured’ while you’re about to explode or are experiencing a strong emotion such as anger or sadness? How did you feel? If I had to guess, you probably weren’t listening to much of what was being said. In fact, the ‘lecture’ may have intensified how you were feeling. That’s because the amygdala (the part of the brain that controls how we feel) takes over, and the part of the brain that helps us to be rational and problem solve does not function as effectively.
To be able to have a conducive conversation with another individual, we need to first ensure that the amygdala is not in control. The way to do this is to first address the emotion being expressed. Acknowledge how your child is feelings and try understanding where this emotion is coming from. When children feel heard and understood, the amygdala calms down and they are then able to use their rational and problem-solving part of brain to have those meaningful conversations we all wish to have with others (including our partners!).
Positive reinforcements have longer lasting effects on our children’s learning.
Praising, complementing, and rewarding them for good and appropriate behaviours can increase the likelihood of them continuing to exhibit these behaviours.
I believe that there is a role of consequences. However, these consequences are the natural consequences one will need to bear for the decisions we make. Assist your child to connect specific consequences to specific behaviour. For example, if a child enjoys throwing things around the house, or drawing on the wall, a natural consequence of that would be to pack their things away or clean up the mess they made. If a child hits and hurts another person, conversations around how they can mend that relationship will help them develop an understanding that their actions can have a negative impact on others.
Actions speak louder than words.
In addition to talking to our children about what is right from wrong, and what is appropriate or inappropriate, they are more likely to act as we do. In other words, we need to ‘walk the talk’ and lead by example. Let’s model the behaviours and values we want our children to learn.
4) Consistency is key
Children love their parents to be consistent as this helps them predict how parents will act.
Consistency means as parents we follow through and do as we say we will.
The following are some resources that you may find beneficial:
The Whole-Brain Child- 12 revolutionary strategies to nurture your child’s developing mind, survive everyday parenting struggles, and help your family thrive. By: Daniel J. Siegel, Tina Payne Bryson
No-Drama Discipline: The Whole-Brain Way to Calm the Chaos and Nurture Your Child’s Developing Mind. Book by Daniel J. Siegel and Tina Payne Bryson.
This blog was written by Dr Aiyuen (Shannon) Choong, Psychologist at Your Mind Matters. Aiyuen is fluent in English and Mandarin, and is passionate about working with children from preschool years through to adolescence.